Home » OA/TOF information » OA/TOF Information for Schools & Nurseries
Home » OA/TOF information » OA/TOF Information for Schools & Nurseries
Please note: It is important for staff, teachers and lunchtime supervisors to meet with parents to discuss the individual child and to draw up a care plan.
In the event of an ambulance being necessary, please provide ambulance crew with the care plan. It is unlikely that they will be familiar with this rare defect and its aftercare.
TOFS has produced a number of resources to help schools & nurseries support children born with OA/TOF.
You may also find these resources (not produced by TOFS) useful.
Healthy Lungs for Life (for Schools)
From the European Lung Foundation (ELF) – a series of resources for schools. They are available for ages 5-7, 7-11 and 11-14 and are in-line with the needs set out in the curriculum.

When Joe was 8, he thought it was important to teach his classmates about his experiences with OA/TOF and why it makes him special. So, he decided to make a wonderful presentation to tell them all about it. Joe did a fantastic job of explaining about his condition and his classmates learned a lot too! Please feel free to download the presentation and adapt it, if you feel it might help you explain OA/TOF to your class.

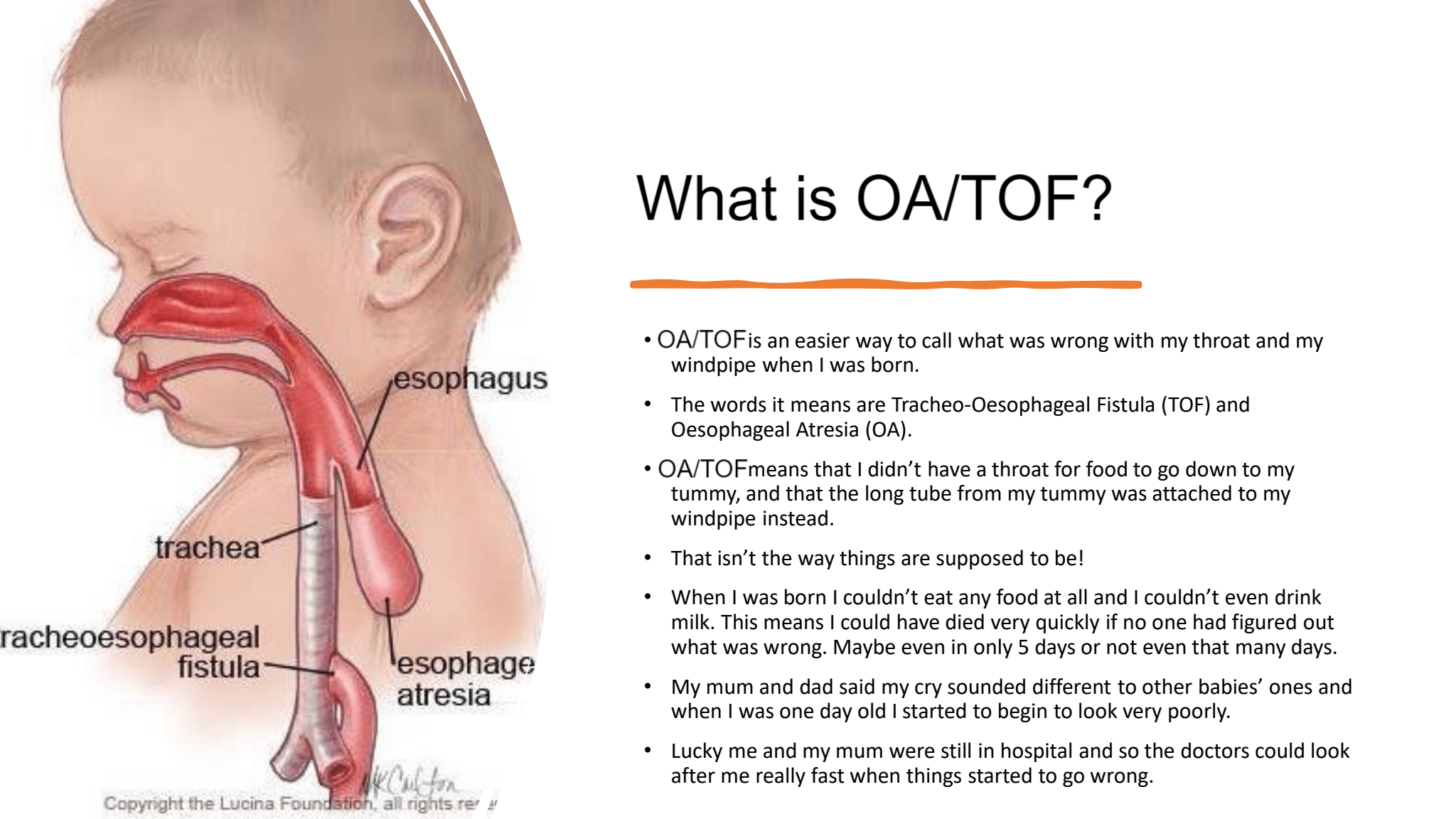




Oesophageal atresia (OA)
In oesophageal atresia, the baby is born with a pouch at the top of its oesophagus (food pipe), which prevents food from reaching the stomach.
Tracheo-oesophageal fistula (TOF)
In tracheo-oesophageal fistula, the bottom end of the baby’s oesophagus is joined to the trachea (windpipe). Without surgical intervention, this causes air to pass from the windpipe to the food pipe and stomach. It can also allow stomach acid to pass into the lungs.
TOF and OA usually occur together but can, less commonly, occur alone. In the vast majority of cases, both of these abnormalities can be corrected in one or more operations taking place within days of birth. After surgery, children who were born with OA/TOF vary in the difficulties they experience, but most will have ongoing feeding and/or respiratory problems.
Children with OA/TOF often have a loud, barking cough, known as the “TOF cough”. It’s caused by a floppiness (tracheomalacia) of part of the trachea (windpipe) and can get worse when a child has a cold or other respiratory problems.
Whilst it can sound alarming, it doesn’t necessarily mean the child is ill.
Read more about Tracheomalacia and the TOF cough.
Children with OA/TOF often have abnormal swallowing mechanisms and will have to learn to cope with their particular feeding problems.
Some children will need to receive tube feeding to make sure they stay healthy.
At first, many will need a special diet, but most will (with their support of their school) cope with school dinners or a packed lunch.
Read more about strictures.
Babies with OA/TOF can experience short periods when they find it hard to breathe, due to a floppy trachea. This is most likely to happen when a child is breathing heavily, for example when coughing or crying. Children usually grow out of this by the age of two and then only a minority of babies suffer severely.
Babies may also experience respiratory problems such as asthma and chest infections. These are treated with inhalers or antibiotic treatments.
Read more about respiratory problems and chest infections.
Children with OA/TOF often experience gastro-oesophageal reflux (GOR).
This is where the acidic stomach contents pass back into the lower oesophagus, causing pain and often reluctance to eat.
Reflux can usually be treated using a combination of practical measures and prescribed medications. Occasionally it requires further surgery.
Read more about gastro-oesophageal reflux.
Carers and parents are encouraged to draw up an Individual Health Care Plan (IHCP) to provide to the education setting, which will outline the specific details of their condition and provisions that will be needed (download a template for schools here and a template for nurseries here).
The school’s role will be to identify if the child requires medical intervention and know the steps to follow.
Some children may have regular medications, such as PPIs and inhalers, which they may need to be given at school. Parents will provide letter written by a GP or paediatrician outlining the need for the medication and its purpose, required dose and dispensing method.
Children may need to have a little bottle of fizzy water or lemonade in the classroom cupboard and school dining hall should it be needed for mild stickies, but this is with agreement between the parents and school.
The school nursing service should be involved in any additional training that is required for staff in the event of food becoming stuck or if any issues should arise relating to the condition.
If possible, it would be helpful for any child born with OA/TOF to be overseen by a lunchtime supervisors or, if necessary have a 1-1 at meal and snack times. If the school does not have funding for this, it is useful that the child knows which lunchtime supervisor they can approach if they get into difficulties.
OA/TOF children do need to be allowed additional time to eat. This may mean going to the lunch hall early. It would also be beneficial for parents to be shown the lunch menu ahead of time so that they can select ‘TOF-friendly’ foods.
Extra gravy, ketchup, sauce and drinks will be required when serving the food. Children born with OA/TOF will need to have extra drinks throughout the day to ensure they have plenty to help them swallow their lunch and snacks.
Parents may need to provide an alternative snack for the school to keep in the cupboard like sundried/ yoghurt coated raisins or fruit winders for days when the supplied fruit is not one they can manage.
For secondary school aged children, lunch passes to allow the pupil to go down to the canteen five minutes early are useful, as lunch breaks tend to be much shorter. Toilet passes are also useful due to drinking more when eating.
Don’t hurry me!
Lunchtime at nursery or school is a noisy, sociable time; most children want to wolf down their food and get outside to play. Children with TOF/OA are no different in this, but they need to eat more slowly and chew their food thoroughly. Please do not try to hurry them.
Don’t distract me!
TOF children need to concentrate on the mechanics of eating more than other children. While it is important that they are not treated differently to their peers, it might occasionally be appropriate to seat them with a couple of understanding friends on a quieter table where they will not be distracted.
Drink up!
Most children with OA/TOF must have access to plenty of drink with all food they eat – even with snacks. The liquid helps the food to pass smoothly into their stomach. They may therefore need to drink more than other children when eating.
I’m full!
TOF children may have small appetites, especially where reflux has been diagnosed. Eating little and often is easier for them than having large meals. It is not advisable to make them eat more than they feel they can.
Don’t embarrass me!
Just like their peers, children with OA/TOF do not like to be made to feel different. Too much fuss can embarrass them. It is very important that as far as possible they join in with normal communal eating and that any extra supervision is low key.
Join TOFS and be a part of the largest community of parents, careers and those born with OA/TOFs in the world. Find out more…
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-advertisement | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Advertisement" category . |
| cookielawinfo-checkbox-analytics | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Analytics" category . |
| cookielawinfo-checkbox-functional | 1 year | The cookie is set by the GDPR Cookie Consent plugin to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Necessary" category . |
| cookielawinfo-checkbox-others | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Others". |
| cookielawinfo-checkbox-performance | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Performance". |
| CookieLawInfoConsent | 1 year | Records the default button state of the corresponding category & the status of CCPA. It works only in coordination with the primary cookie. |
| elementor | never | This cookie is used by the website's WordPress theme. It allows the website owner to implement or change the website's content in real-time. |
| enforce_policy | 1 year | PayPal sets this cookie for secure transactions. |
| ts | 3 years | PayPal sets this cookie to enable secure transactions through PayPal. |
| ts_c | 3 years | PayPal sets this cookie to make safe payments through PayPal. |
| Cookie | Duration | Description |
|---|---|---|
| aka_debug | session | Vimeo sets this cookie which is essential for the website to play video functionality. |
| nsid | session | This cookie is set by the provider PayPal to enable the PayPal payment service in the website. |
| player | 1 year | Vimeo uses this cookie to save the user's preferences when playing embedded videos from Vimeo. |
| tsrce | 3 days | PayPal sets this cookie to enable the PayPal payment service in the website. |
| x-pp-s | session | PayPal sets this cookie to process payments on the site. |
| Cookie | Duration | Description |
|---|---|---|
| l7_az | 30 minutes | This cookie is necessary for the PayPal login-function on the website. |
| sync_active | never | This cookie is set by Vimeo and contains data on the visitor's video-content preferences, so that the website remembers parameters such as preferred volume or video quality. |
| Cookie | Duration | Description |
|---|---|---|
| _ga | 2 years | The _ga cookie, installed by Google Analytics, calculates visitor, session and campaign data and also keeps track of site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognize unique visitors. |
| _gat_UA-51564864-7 | 1 minute | A variation of the _gat cookie set by Google Analytics and Google Tag Manager to allow website owners to track visitor behaviour and measure site performance. The pattern element in the name contains the unique identity number of the account or website it relates to. |
| _gcl_au | 3 months | Provided by Google Tag Manager to experiment advertisement efficiency of websites using their services. |
| _gid | 1 day | Installed by Google Analytics, _gid cookie stores information on how visitors use a website, while also creating an analytics report of the website's performance. Some of the data that are collected include the number of visitors, their source, and the pages they visit anonymously. |
| _hjAbsoluteSessionInProgress | 30 minutes | Hotjar sets this cookie to detect the first pageview session of a user. This is a True/False flag set by the cookie. |
| _hjFirstSeen | 30 minutes | Hotjar sets this cookie to identify a new user’s first session. It stores a true/false value, indicating whether it was the first time Hotjar saw this user. |
| _hjIncludedInPageviewSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's pageview limit. |
| _hjIncludedInSessionSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's daily session limit. |
| CONSENT | 2 years | YouTube sets this cookie via embedded youtube-videos and registers anonymous statistical data. |
| vuid | 2 years | Vimeo installs this cookie to collect tracking information by setting a unique ID to embed videos to the website. |
| Cookie | Duration | Description |
|---|---|---|
| VISITOR_INFO1_LIVE | 5 months 27 days | A cookie set by YouTube to measure bandwidth that determines whether the user gets the new or old player interface. |
| YSC | session | YSC cookie is set by Youtube and is used to track the views of embedded videos on Youtube pages. |
| yt-remote-connected-devices | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt-remote-device-id | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt.innertube::nextId | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| yt.innertube::requests | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| Cookie | Duration | Description |
|---|---|---|
| _hjSession_2528865 | 30 minutes | No description |
| _hjSessionUser_2528865 | 1 year | No description |
| LANG | 9 hours | No description |