Home » What is OA/TOF? » Surgery for OA/TOF » Long gap OA – delayed primary anastomosis
Home » What is OA/TOF? » Surgery for OA/TOF » Long gap OA – delayed primary anastomosis
Most babies born with oesophageal atresia (OA) undergo a primary repair within the first few days of life. However, approximately 10% of babies have a gap between the upper and lower ends of the oesophagus which is too long for a primary repair.
These babies have long gap oesophageal atresia.
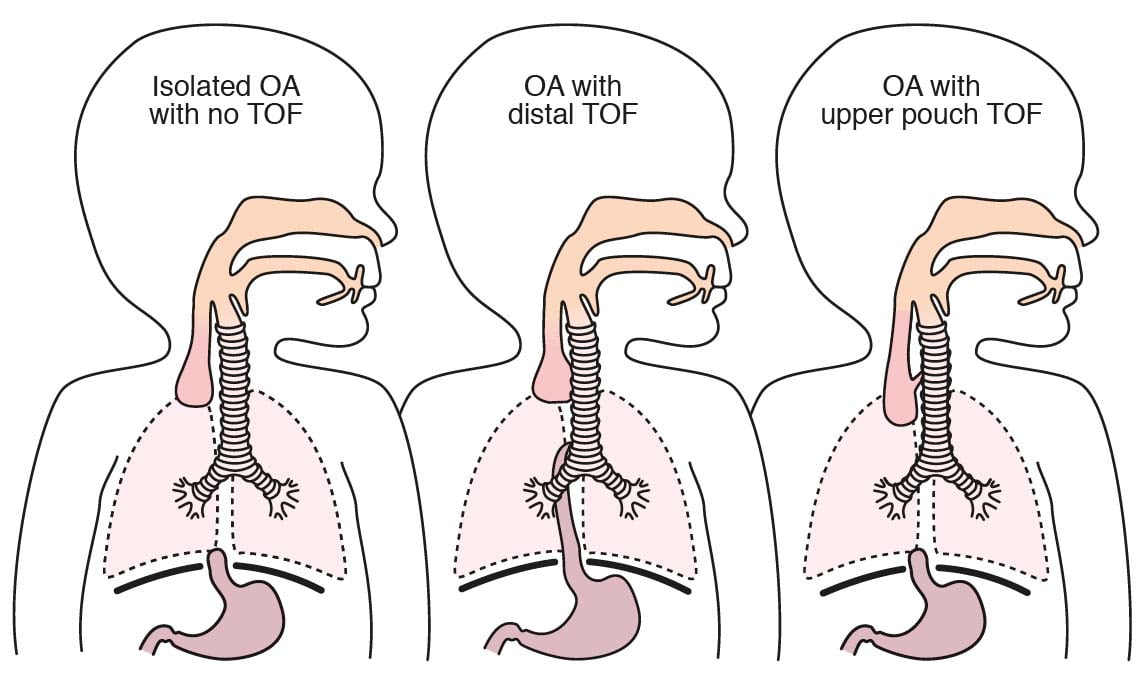
Long gap oesophageal atresia can occur in babies with a distal tracheo-oesophageal fistula (TOF), but is much more common (80%) in babies born with isolated OA, without a distal TOF. Around 10% of babies with long gap OA have an upper pouch TOF instead of a distal TOF.
There are several treatment options for babies with long gap OA.
The diagnosis of OA is confirmed shortly after birth when a doctor or nurse attempts to pass a feeding tube through the mouth or nose, down the oesophagus, and into the stomach.
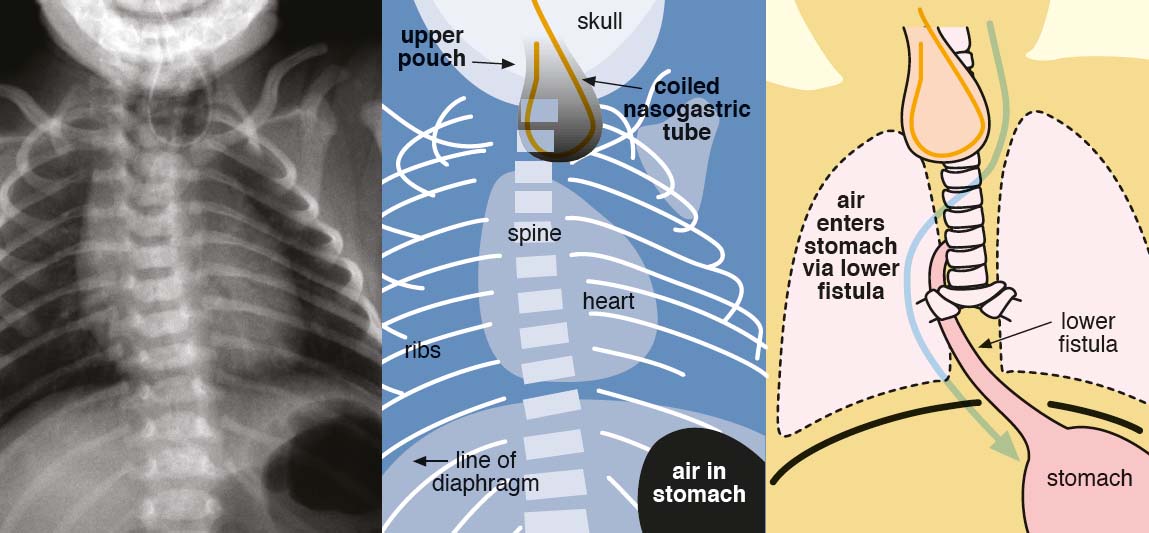
If the lower oesophagus is connected to the trachea (a distal tracheo-oesophageal fistula), air can be seen in the stomach on the x-ray.

If the initial chest x-ray confirms oesophageal atresia but there is no air in the stomach, then the usual explanation is that there is isolated oesophageal atresia with no distal TOF.
Once a long gap OA diagnosis has been made, oral feeding must not occur.
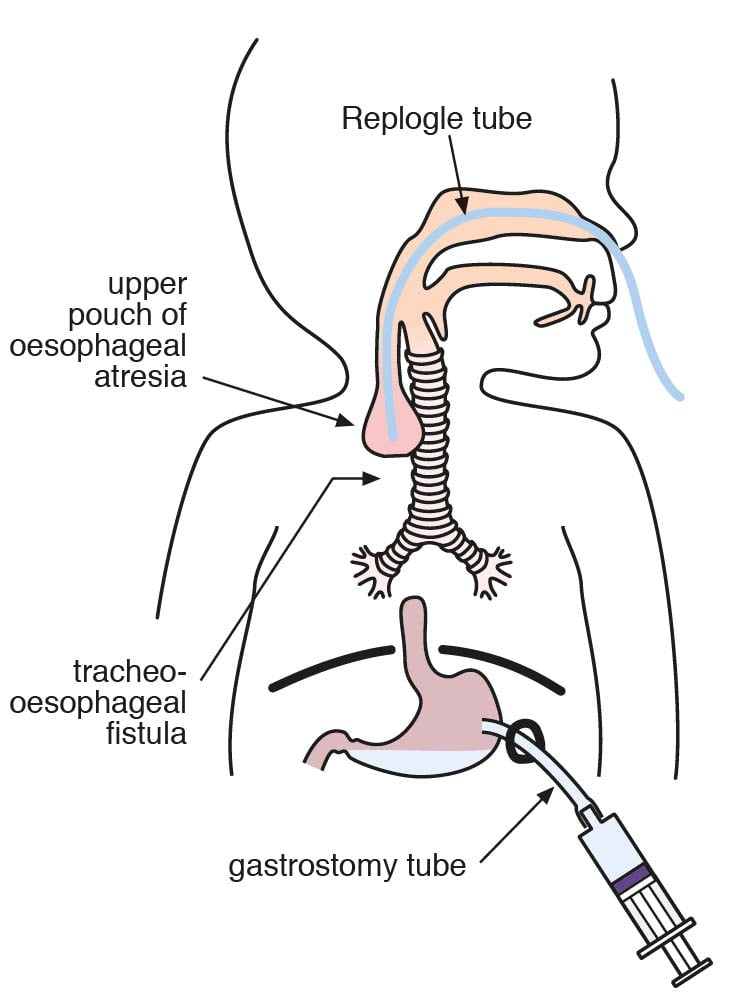
A tube called a Replogle tube is inserted into the upper oesophagus to hoover out saliva. This is necessary to prevent saliva spilling over into the airway and causing a chest infection (aspiration pneumonia).
A gastrostomy feeding tube is stitched into the stomach within the first few days of life with an operation on the abdomen. Milk feeds are started through the gastrostomy using either the mother’s expressed breast milk (EBM) or formula milk.
Some surgeons use a camera (a bronchoscope) in the trachea to check that there is no connection between the upper oesophagus and the trachea (an upper pouch TOF). This is rare and some surgeons delay this until the baby is bigger. If there is an upper pouch TOF this will have to be divided at some stage which usually involves an operation on the neck.
With a gastrostomy tube in place for feeding and a Replogle tube to prevent aspiration of saliva into the lungs, the baby is in a safe position to let them and their oesophagus grow.
The Replogle tube must be kept on continuous suction and flushed with small volumes of water every 15-30 minutes to prevent blockage.
The baby cannot feed by mouth although some surgeons allow a dummy. Sham feeding may also be recommended.
Despite all of this chest infections are fairly common in babies on Replogle suction. Chest infections are not usually dangerous and does not cause long term damage but they do make babies poorly and often put them into oxygen.
Waiting for the oesophagus to grow or, to be more accurate, waiting for the gap to narrow, takes weeks to months. This is always a hugely frustrating time for parents.
During this time, your baby has to remain in hospital and cannot feed. Worse than that, the baby forgets how to feed. So, why do they do this?
The reason is because in most babies the gap will narrow over the first few months to the point that it becomes possible to join the two ends of the oesophagus together.
This is procedure is called a delayed primary anastomosis – delayed because of the wait, primary because it is the first operation on the oesophagus (at least in a baby with isolated OA) and anastomosis meaning the join.
Published by TOFS, The TOF Book is the must have guide for anyone affected by, or caring for someone with OA/TOF.
With contributions from medical experts, the TOF Book contains chapters on every aspect of OA/TOF and VACTERL condition, from infancy to adulthood all presented in an easy-to-understand format.
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-advertisement | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Advertisement" category . |
| cookielawinfo-checkbox-analytics | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Analytics" category . |
| cookielawinfo-checkbox-functional | 1 year | The cookie is set by the GDPR Cookie Consent plugin to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Necessary" category . |
| cookielawinfo-checkbox-others | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Others". |
| cookielawinfo-checkbox-performance | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Performance". |
| CookieLawInfoConsent | 1 year | Records the default button state of the corresponding category & the status of CCPA. It works only in coordination with the primary cookie. |
| elementor | never | This cookie is used by the website's WordPress theme. It allows the website owner to implement or change the website's content in real-time. |
| enforce_policy | 1 year | PayPal sets this cookie for secure transactions. |
| ts | 3 years | PayPal sets this cookie to enable secure transactions through PayPal. |
| ts_c | 3 years | PayPal sets this cookie to make safe payments through PayPal. |
| Cookie | Duration | Description |
|---|---|---|
| aka_debug | session | Vimeo sets this cookie which is essential for the website to play video functionality. |
| nsid | session | This cookie is set by the provider PayPal to enable the PayPal payment service in the website. |
| player | 1 year | Vimeo uses this cookie to save the user's preferences when playing embedded videos from Vimeo. |
| tsrce | 3 days | PayPal sets this cookie to enable the PayPal payment service in the website. |
| x-pp-s | session | PayPal sets this cookie to process payments on the site. |
| Cookie | Duration | Description |
|---|---|---|
| l7_az | 30 minutes | This cookie is necessary for the PayPal login-function on the website. |
| sync_active | never | This cookie is set by Vimeo and contains data on the visitor's video-content preferences, so that the website remembers parameters such as preferred volume or video quality. |
| Cookie | Duration | Description |
|---|---|---|
| _ga | 2 years | The _ga cookie, installed by Google Analytics, calculates visitor, session and campaign data and also keeps track of site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognize unique visitors. |
| _gat_UA-51564864-7 | 1 minute | A variation of the _gat cookie set by Google Analytics and Google Tag Manager to allow website owners to track visitor behaviour and measure site performance. The pattern element in the name contains the unique identity number of the account or website it relates to. |
| _gcl_au | 3 months | Provided by Google Tag Manager to experiment advertisement efficiency of websites using their services. |
| _gid | 1 day | Installed by Google Analytics, _gid cookie stores information on how visitors use a website, while also creating an analytics report of the website's performance. Some of the data that are collected include the number of visitors, their source, and the pages they visit anonymously. |
| _hjAbsoluteSessionInProgress | 30 minutes | Hotjar sets this cookie to detect the first pageview session of a user. This is a True/False flag set by the cookie. |
| _hjFirstSeen | 30 minutes | Hotjar sets this cookie to identify a new user’s first session. It stores a true/false value, indicating whether it was the first time Hotjar saw this user. |
| _hjIncludedInPageviewSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's pageview limit. |
| _hjIncludedInSessionSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's daily session limit. |
| CONSENT | 2 years | YouTube sets this cookie via embedded youtube-videos and registers anonymous statistical data. |
| vuid | 2 years | Vimeo installs this cookie to collect tracking information by setting a unique ID to embed videos to the website. |
| Cookie | Duration | Description |
|---|---|---|
| VISITOR_INFO1_LIVE | 5 months 27 days | A cookie set by YouTube to measure bandwidth that determines whether the user gets the new or old player interface. |
| YSC | session | YSC cookie is set by Youtube and is used to track the views of embedded videos on Youtube pages. |
| yt-remote-connected-devices | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt-remote-device-id | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt.innertube::nextId | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| yt.innertube::requests | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| Cookie | Duration | Description |
|---|---|---|
| _hjSession_2528865 | 30 minutes | No description |
| _hjSessionUser_2528865 | 1 year | No description |
| LANG | 9 hours | No description |