Home » What is OA/TOF? » Surgery for OA/TOF » Post operative procedures » Gastric transposition
Home » What is OA/TOF? » Surgery for OA/TOF » Post operative procedures » Gastric transposition
The oesophagus is usually the best tube to convey food from the mouth to the stomach. When the oesophagus is absent or badly diseased, oesophageal replacement may be required.
Gastric transposition (also called gastric pull-up or stomach pull-up) involves moving the whole stomach upwards into the chest to join onto the top end of the oesophagus in the neck. This is probably the most commonly used technique for oesophageal replacement in children in the UK at present.

The question most parents ask when a gastric transposition is proposed is: “How can a child manage without a stomach in the abdomen?”
The answer is that they manage just fine.
When the stomach is in the chest, it doesn’t really function as a reservoir to store food – it works more as a tube, or conduit, to convey liquids and solids to the small bowel.
The normal function of the stomach is to store food and liquid and release it, a little at a time, into the small bowel where it is digested and absorbed.
You don’t need a full stomach to feel full.
The feeling of fullness, or hunger, arises within the brain and is mainly due to the effects of gut hormones (substances released from the gut into the bloodstream) which act on the brain. This feedback system works normally whether the stomach is in the abdomen or the chest. The stomach is a robust organ with a very good blood supply. It sits in the top left hand side of the abdomen and connects with the duodenum (the first part of the small bowel).
This means that the stomach can be mobilised relatively easily, pulled up through the back of the chest and joined to the upper oesophagus in the neck.
Advantages of this technique are:
Gastric transposition operations have been performed in the neonatal period. Most surgeons however recommend waiting until sometime later in the first year. The decision depends on many factors including:
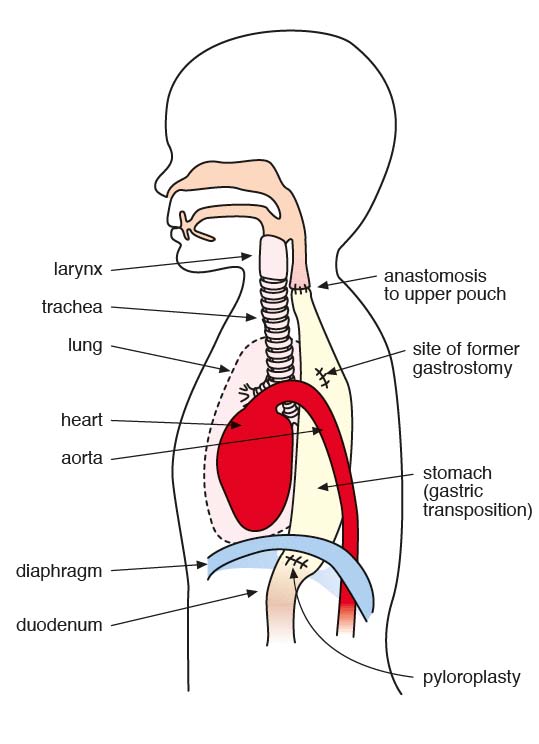
The operation of gastric transposition involves moving (transposing) the whole stomach from the abdomen into the chest and joining the top of the stomach onto the oesophagus in the neck.
There are two consequences of moving the stomach into the chest:
The operation takes between 4-8 hours. At the end of the operation the patient is transferred to the intensive care unit (ICU)asleep and ventilated.
It is usually necessary to ventilate a baby for several days after surgery which involves heavy sedation and muscle relaxant drugs. The surgical and ICU team monitor the baby closely during this period and look at many different factors to decide when they are ready to come off the ventilator. These factors include oxygen requirements, ventilation pressures and fluid balance.
Milk feeds can usually be started through the jejunostomy after 48-72 hours.
Published by TOFS, The TOF Book is the must have guide for anyone affected by, or caring for someone with OA/TOF.
With contributions from medical experts, the TOF Book contains chapters on every aspect of OA/TOF and VACTERL condition, from infancy to adulthood all presented in an easy-to-understand format.
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-advertisement | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Advertisement" category . |
| cookielawinfo-checkbox-analytics | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Analytics" category . |
| cookielawinfo-checkbox-functional | 1 year | The cookie is set by the GDPR Cookie Consent plugin to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Necessary" category . |
| cookielawinfo-checkbox-others | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Others". |
| cookielawinfo-checkbox-performance | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Performance". |
| CookieLawInfoConsent | 1 year | Records the default button state of the corresponding category & the status of CCPA. It works only in coordination with the primary cookie. |
| elementor | never | This cookie is used by the website's WordPress theme. It allows the website owner to implement or change the website's content in real-time. |
| enforce_policy | 1 year | PayPal sets this cookie for secure transactions. |
| ts | 3 years | PayPal sets this cookie to enable secure transactions through PayPal. |
| ts_c | 3 years | PayPal sets this cookie to make safe payments through PayPal. |
| Cookie | Duration | Description |
|---|---|---|
| aka_debug | session | Vimeo sets this cookie which is essential for the website to play video functionality. |
| nsid | session | This cookie is set by the provider PayPal to enable the PayPal payment service in the website. |
| player | 1 year | Vimeo uses this cookie to save the user's preferences when playing embedded videos from Vimeo. |
| tsrce | 3 days | PayPal sets this cookie to enable the PayPal payment service in the website. |
| x-pp-s | session | PayPal sets this cookie to process payments on the site. |
| Cookie | Duration | Description |
|---|---|---|
| l7_az | 30 minutes | This cookie is necessary for the PayPal login-function on the website. |
| sync_active | never | This cookie is set by Vimeo and contains data on the visitor's video-content preferences, so that the website remembers parameters such as preferred volume or video quality. |
| Cookie | Duration | Description |
|---|---|---|
| _ga | 2 years | The _ga cookie, installed by Google Analytics, calculates visitor, session and campaign data and also keeps track of site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognize unique visitors. |
| _gat_UA-51564864-7 | 1 minute | A variation of the _gat cookie set by Google Analytics and Google Tag Manager to allow website owners to track visitor behaviour and measure site performance. The pattern element in the name contains the unique identity number of the account or website it relates to. |
| _gcl_au | 3 months | Provided by Google Tag Manager to experiment advertisement efficiency of websites using their services. |
| _gid | 1 day | Installed by Google Analytics, _gid cookie stores information on how visitors use a website, while also creating an analytics report of the website's performance. Some of the data that are collected include the number of visitors, their source, and the pages they visit anonymously. |
| _hjAbsoluteSessionInProgress | 30 minutes | Hotjar sets this cookie to detect the first pageview session of a user. This is a True/False flag set by the cookie. |
| _hjFirstSeen | 30 minutes | Hotjar sets this cookie to identify a new user’s first session. It stores a true/false value, indicating whether it was the first time Hotjar saw this user. |
| _hjIncludedInPageviewSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's pageview limit. |
| _hjIncludedInSessionSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's daily session limit. |
| CONSENT | 2 years | YouTube sets this cookie via embedded youtube-videos and registers anonymous statistical data. |
| vuid | 2 years | Vimeo installs this cookie to collect tracking information by setting a unique ID to embed videos to the website. |
| Cookie | Duration | Description |
|---|---|---|
| VISITOR_INFO1_LIVE | 5 months 27 days | A cookie set by YouTube to measure bandwidth that determines whether the user gets the new or old player interface. |
| YSC | session | YSC cookie is set by Youtube and is used to track the views of embedded videos on Youtube pages. |
| yt-remote-connected-devices | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt-remote-device-id | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt.innertube::nextId | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| yt.innertube::requests | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| Cookie | Duration | Description |
|---|---|---|
| _hjSession_2528865 | 30 minutes | No description |
| _hjSessionUser_2528865 | 1 year | No description |
| LANG | 9 hours | No description |