Home » What is OA/TOF? » Surgery for OA/TOF » Post operative procedures » Oesophageal dilatation
Home » What is OA/TOF? » Surgery for OA/TOF » Post operative procedures » Oesophageal dilatation
An oesophageal dilatation is a stretching of an anastomotic stricture.
The terms dilatation and dilation are often used interchangeably; either way they mean a stretch of the stricture.
This procedure may be performed in an operating theatre while the doctor (surgeon or gastroenterologist) views the process directly with the endoscope (medical telescope) in the oesophagus – or in an x-ray (radiology) department with the doctor (radiologist) viewing the procedure indirectly using x-ray screening.
The traditional way of achieving a dilatation or stretch was with a bougie (pronounced ‘boojee’) which is a soft pliable plastic rod with a tapered end.
This is passed down the oesophagus, either viewed using a rigid oesophagoscope or done blind by feel (which requires a lot of experience). Some surgeons regard bougies as safe and effective, while others believe they create a shearing force and may increase the risk of oesophageal perforation (rupture).
Balloon catheter dilatation is considered safer as a radial or tangential force is applied to the oesophagus – rather than the shearing force applied by bougie. It may therefore be associated with a lesser risk of oesophageal perforation or rupture.
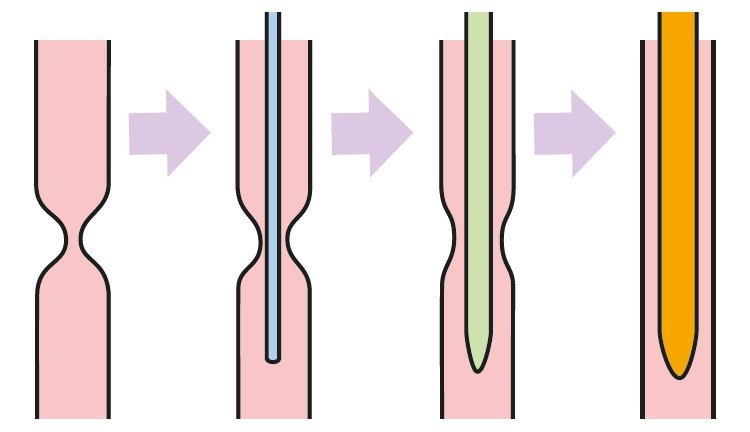
Dilatations are usually performed with a balloon that can be passed down the operating channel of a flexible endoscope, or alongside the endoscope. If the stricture is very tight and only a pinhole opening is visible, the safest manoeuvre is to first pass a thin flexible guidewire (visible on x-ray screening) down through the stricture, then the balloon catheter can be pushed over it.
Injection of an x-ray dye into the balloon allows it to be seen on x-ray screen.
When inflated to a certain diameter and pressure, the balloon will be indented by the stricture and be seen as a clear ‘waist’ in the balloon as visualised on the x-ray screen.
The maximum safe pressure and diameter is gauged by the surgeon, but the patient’s thumb diameter is an approximate guide to the expected diameter of their oesophagus.
A typical routine is to inflate the balloon for two minutes at one pressure and diameter, then a further two minutes at a greater diameter, followed by a final (third) diameter for two minutes. The increments of diameter are generally 1mm each time.
This has not been formally proven to be the best routine, but is widely practised. The rule of three has been taken from adult practice and applied to children as follows:
Increases greater than this may be used by individual surgeons, according to the nature of the patient’s difficulties.
Dilatation may become necessary within a few weeks after surgery and may need to be repeated on a regular basis.

| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-advertisement | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Advertisement" category . |
| cookielawinfo-checkbox-analytics | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Analytics" category . |
| cookielawinfo-checkbox-functional | 1 year | The cookie is set by the GDPR Cookie Consent plugin to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to record the user consent for the cookies in the "Necessary" category . |
| cookielawinfo-checkbox-others | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Others". |
| cookielawinfo-checkbox-performance | 1 year | Set by the GDPR Cookie Consent plugin, this cookie is used to store the user consent for cookies in the category "Performance". |
| CookieLawInfoConsent | 1 year | Records the default button state of the corresponding category & the status of CCPA. It works only in coordination with the primary cookie. |
| elementor | never | This cookie is used by the website's WordPress theme. It allows the website owner to implement or change the website's content in real-time. |
| enforce_policy | 1 year | PayPal sets this cookie for secure transactions. |
| ts | 3 years | PayPal sets this cookie to enable secure transactions through PayPal. |
| ts_c | 3 years | PayPal sets this cookie to make safe payments through PayPal. |
| Cookie | Duration | Description |
|---|---|---|
| aka_debug | session | Vimeo sets this cookie which is essential for the website to play video functionality. |
| nsid | session | This cookie is set by the provider PayPal to enable the PayPal payment service in the website. |
| player | 1 year | Vimeo uses this cookie to save the user's preferences when playing embedded videos from Vimeo. |
| tsrce | 3 days | PayPal sets this cookie to enable the PayPal payment service in the website. |
| x-pp-s | session | PayPal sets this cookie to process payments on the site. |
| Cookie | Duration | Description |
|---|---|---|
| l7_az | 30 minutes | This cookie is necessary for the PayPal login-function on the website. |
| sync_active | never | This cookie is set by Vimeo and contains data on the visitor's video-content preferences, so that the website remembers parameters such as preferred volume or video quality. |
| Cookie | Duration | Description |
|---|---|---|
| _ga | 2 years | The _ga cookie, installed by Google Analytics, calculates visitor, session and campaign data and also keeps track of site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognize unique visitors. |
| _gat_UA-51564864-7 | 1 minute | A variation of the _gat cookie set by Google Analytics and Google Tag Manager to allow website owners to track visitor behaviour and measure site performance. The pattern element in the name contains the unique identity number of the account or website it relates to. |
| _gcl_au | 3 months | Provided by Google Tag Manager to experiment advertisement efficiency of websites using their services. |
| _gid | 1 day | Installed by Google Analytics, _gid cookie stores information on how visitors use a website, while also creating an analytics report of the website's performance. Some of the data that are collected include the number of visitors, their source, and the pages they visit anonymously. |
| _hjAbsoluteSessionInProgress | 30 minutes | Hotjar sets this cookie to detect the first pageview session of a user. This is a True/False flag set by the cookie. |
| _hjFirstSeen | 30 minutes | Hotjar sets this cookie to identify a new user’s first session. It stores a true/false value, indicating whether it was the first time Hotjar saw this user. |
| _hjIncludedInPageviewSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's pageview limit. |
| _hjIncludedInSessionSample | 2 minutes | Hotjar sets this cookie to know whether a user is included in the data sampling defined by the site's daily session limit. |
| CONSENT | 2 years | YouTube sets this cookie via embedded youtube-videos and registers anonymous statistical data. |
| vuid | 2 years | Vimeo installs this cookie to collect tracking information by setting a unique ID to embed videos to the website. |
| Cookie | Duration | Description |
|---|---|---|
| VISITOR_INFO1_LIVE | 5 months 27 days | A cookie set by YouTube to measure bandwidth that determines whether the user gets the new or old player interface. |
| YSC | session | YSC cookie is set by Youtube and is used to track the views of embedded videos on Youtube pages. |
| yt-remote-connected-devices | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt-remote-device-id | never | YouTube sets this cookie to store the video preferences of the user using embedded YouTube video. |
| yt.innertube::nextId | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| yt.innertube::requests | never | This cookie, set by YouTube, registers a unique ID to store data on what videos from YouTube the user has seen. |
| Cookie | Duration | Description |
|---|---|---|
| _hjSession_2528865 | 30 minutes | No description |
| _hjSessionUser_2528865 | 1 year | No description |
| LANG | 9 hours | No description |